
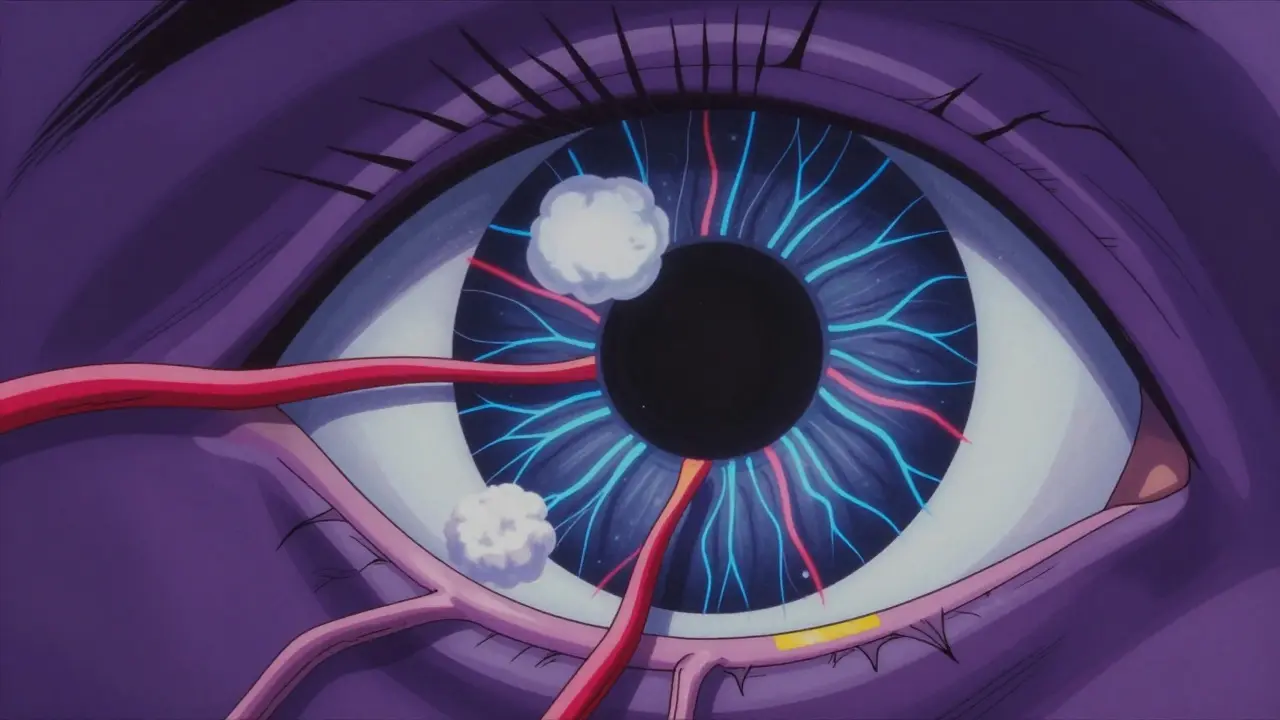
High blood pressure is often called the "silent killer" because it rarely shows symptoms until significant damage has occurred. But there is one place where you can actually see the effects of uncontrolled hypertension with your own eyes-literally. The retina, the light-sensitive tissue at the back of your eye, contains some of the smallest and most delicate blood vessels in your body. When your blood pressure stays too high for too long, these tiny vessels take a beating. This condition is known as hypertensive retinopathy, which is damage to the retinal blood vessels caused by chronically elevated systemic blood pressure. It serves as a critical warning sign that your cardiovascular system is under severe stress.
You might not feel any pain or notice blurry vision in the early stages. In fact, many people walk around with damaged retinal vessels without knowing it. However, this eye condition is more than just an ophthalmic issue; it is a direct window into your overall vascular health. If left unchecked, hypertensive retinopathy can lead to permanent vision loss, stroke, heart attack, and kidney failure. Understanding how high blood pressure affects your eyes is the first step toward protecting both your sight and your life.
The Silent Progression: Stages of Retinal Damage
Doctors do not guess when diagnosing this condition. They use a standardized grading system called the Keith-Wagener-Barker (KWB) classification, which is a four-stage system used to grade the severity of hypertensive retinopathy based on specific retinal changes. This system helps medical professionals determine how advanced the damage is and how urgently treatment is needed. The progression typically follows a predictable path if blood pressure remains uncontrolled.
- Grade 1: This is the mildest form. You will see mild narrowing of the retinal arteries. There are no hemorrhages or exudates yet. At this stage, vision is usually unaffected, but the vessel walls have begun to thicken due to constant high pressure.
- Grade 2: The narrowing becomes more pronounced. You may start to see arteriovenous nicking, which occurs when a hardened artery compresses a vein underneath it at their crossing point. This indicates that the arterial walls have become stiff and rigid.
- Grade 3: This is where things get serious. The blood-retinal barrier breaks down, leading to leakage. Signs include retinal hemorrhages (bleeding in the eye), cotton wool spots (fluffy white patches indicating nerve fiber layer infarction), and hard exudates (yellowish deposits of leaked lipids).
- Grade 4: This is the most severe stage, often associated with malignant hypertension. It includes all signs from Grade 3 plus optic disc swelling (also known as papilledema), which is swelling of the optic nerve head due to severely elevated intracranial or intraocular pressure. This is a medical emergency.
Research shows that approximately 22% of patients with uncontrolled hypertension show Grade 1 changes after just three years. By the time you reach Grade 4, the risk of stroke increases by 78%. The key takeaway here is that early detection matters immensely. Once you see cotton wool spots or hemorrhages, the damage is already significant.
Why Your Retina Matters More Than You Think
You might wonder why an eye doctor’s findings should concern your cardiologist. The answer lies in anatomy. The retina is the only place in the human body where doctors can directly visualize blood vessels without surgery. Because these vessels share similar characteristics with those in your brain, heart, and kidneys, changes in the retina strongly predict systemic disease.
Studies indicate that patients with arteriovenous nicking and optic disc swelling face a 3.2 times higher risk of stroke compared to those without these signs. Furthermore, the presence of hypertensive retinopathy correlates with a 2.5 times increased risk of cardiovascular events. This means your eye exam is not just about checking your prescription; it is a vital assessment of your entire circulatory system.
Consider the data from the CDC: roughly 13.9% of U.S. adults have Stage 2 hypertension (systolic BP ≥140 mmHg or diastolic BP ≥90 mmHg). That translates to millions of people walking around with potentially damaging pressure levels. Many of them do not know they are at risk until an eye exam reveals the truth. The retina acts as an early warning system, often showing damage before other organs like the kidneys or heart fail.
Symptoms: What You Might Actually See
Here is the tricky part: you probably won’t feel anything in the beginning. According to clinical data, 68% of patients with Grade 1-2 hypertensive retinopathy report no visual symptoms at all. The damage is happening silently behind the scenes. However, as the condition progresses to Grade 3 and 4, symptoms become impossible to ignore.
Common complaints include blurred vision, double vision, and sudden vision loss. Some patients describe a "curtain-like" effect where parts of their visual field go dark. This often happens during hypertensive emergencies when blood pressure spikes above 180/120 mmHg. Patient accounts from online communities reveal stories of waking up with dark spots in central vision or experiencing severe headaches accompanied by visual disturbances.
If you experience sudden changes in vision, especially if you have a history of high blood pressure, do not wait. These symptoms suggest acute damage to the macula or optic nerve. Immediate medical attention can prevent permanent blindness. Remember, the absence of symptoms does not mean the absence of disease.
Diagnosis and Modern Detection Tools
Diagnosing hypertensive retinopathy requires a comprehensive dilated eye exam. An ophthalmologist uses a fundoscope to look directly at the retina. They check for the specific signs mentioned earlier: narrowing, nicking, hemorrhages, and swelling. Today, technology has made this process even more precise.
Optical Coherence Tomography (OCT) is now widely used. This non-invasive imaging test provides cross-sectional images of the retina, allowing doctors to measure thickness changes with incredible accuracy. In exudative phases, OCT can detect retinal thickness increases of 10-15%, confirming fluid leakage. Additionally, AI-assisted retinal imaging systems, such as IDx-DR, are improving diagnosis accuracy from 75% to 92%. These tools help identify subtle changes that the human eye might miss.
The American Academy of Ophthalmology recommends that anyone with hypertension undergo regular eye exams. For patients with stable, controlled blood pressure, an annual exam is sufficient. However, if you have resistant hypertension (BP >140/90 mmHg despite taking three medications), guidelines now suggest screening every six months. Early detection through these methods allows for timely intervention, preventing progression to sight-threatening stages.
Treatment and Management Strategies
There is no specific medication that cures hypertensive retinopathy directly. The treatment focuses entirely on controlling your blood pressure. Lowering your systolic and diastolic numbers reduces the strain on your retinal vessels, allowing them to heal and preventing further damage.
In acute cases, such as malignant hypertension with papilledema, rapid blood pressure reduction is critical. Clinical studies show that reducing systolic BP by 25 mmHg within 24-48 hours resolves acute retinal changes in 65% of cases. However, this must be done carefully under medical supervision to avoid causing ischemia (lack of blood flow) to other organs.
For long-term management, lifestyle changes play a huge role. Reducing salt intake, exercising regularly, maintaining a healthy weight, and quitting smoking are essential. Medication adherence is equally important. Studies show that 70% of patients stick to their medication regimens when they understand the connection between their pills and their eye health. Programs like the American Heart Association’s "Check. Change. Control." initiative have proven effective in improving patient compliance.
Vision improvement typically begins within 7-10 days of effective blood pressure control. However, if macular damage has occurred, recovery may take 3-6 months, and some patients may experience permanent visual field defects. This underscores the importance of prevention over cure.
Risk Factors and Who Is Most Vulnerable
Not everyone with high blood pressure develops hypertensive retinopathy. Several factors increase your risk. Duration and severity matter significantly. Research demonstrates a direct correlation between retinopathy incidence and systolic BP >160 mmHg sustained for more than five years. Even mild hypertension (systolic 130-139 mmHg) can cause damage if left untreated for a decade or more.
Certain groups are at higher risk. African Americans tend to develop hypertension earlier and more severely than other ethnic groups, increasing their vulnerability to retinal complications. Diabetics face a compounded risk; having both diabetes and hypertension increases the likelihood of permanent vision loss by 4.7 times. Age also plays a role, as blood vessels naturally lose elasticity over time, making them more susceptible to pressure-induced damage.
Genetics may also be involved. The NIH’s ongoing RETINA-HTN study is investigating genetic markers that predict susceptibility to hypertensive retinopathy. Preliminary data suggests that certain single-nucleotide polymorphisms could identify high-risk individuals before symptoms appear. While this research is still emerging, it highlights the complex interplay between biology and environment in eye health.
Prevention: Protecting Your Vision Before It’s Too Late
The best way to treat hypertensive retinopathy is to prevent it. Start by monitoring your blood pressure at home. Use a validated upper-arm cuff monitor and take readings twice daily for two weeks to establish a baseline. Share this data with your doctor. Knowing your numbers empowers you to make informed decisions about your health.
Eat a heart-healthy diet rich in fruits, vegetables, whole grains, and lean proteins. The DASH (Dietary Approaches to Stop Hypertension) diet has been clinically proven to lower blood pressure effectively. Limit processed foods, which are often loaded with sodium. Aim for less than 2,300 mg of sodium per day, or ideally 1,500 mg if you have existing hypertension.
Stay active. Regular aerobic exercise, such as brisk walking, swimming, or cycling, strengthens your heart and improves circulation. Aim for at least 150 minutes of moderate-intensity activity per week. Manage stress through techniques like meditation, deep breathing, or yoga, as chronic stress contributes to elevated blood pressure.
Finally, never skip your eye exams. Even if your vision seems perfect, a dilated exam can reveal hidden damage. Ask your optometrist or ophthalmologist specifically about hypertensive retinopathy during your visit. By taking these proactive steps, you protect not only your eyes but also your heart, brain, and kidneys.
Can hypertensive retinopathy be reversed?
In early stages (Grade 1-2), controlling blood pressure can halt progression and allow some healing. However, advanced damage like cotton wool spots or optic disc swelling may result in permanent vision loss. Early intervention is key to preserving sight.
How often should I get my eyes checked if I have high blood pressure?
If your blood pressure is well-controlled, an annual dilated eye exam is recommended. If you have resistant hypertension or existing retinopathy, your doctor may advise exams every six months to monitor for changes.
What are the symptoms of Grade 4 hypertensive retinopathy?
Symptoms include severe blurred vision, sudden vision loss, double vision, and headaches. Optic disc swelling (papilledema) is present, indicating malignant hypertension. This is a medical emergency requiring immediate care.
Does low blood pressure affect the eyes?
While hypertensive retinopathy is caused by high blood pressure, extremely low blood pressure can reduce blood flow to the retina, potentially causing temporary vision dimming or blackouts. However, it does not cause the same structural damage as hypertension.
Is hypertensive retinopathy common in young people?
It is less common in younger individuals unless they have secondary causes of hypertension, such as kidney disease or hormonal disorders. However, rising rates of obesity and poor diet are increasing hypertension prevalence among youth, raising concerns about future eye health.
Nicholas Bowling
June 4, 2026 AT 11:53Jay Foreman
June 5, 2026 AT 21:14Cathy N
June 6, 2026 AT 05:46Adelaide Motata
June 6, 2026 AT 17:28Mike Crump
June 7, 2026 AT 20:22Samantha Arbuckle
June 8, 2026 AT 08:25Stephanie Francis
June 9, 2026 AT 18:21Daniel Tremblay
June 11, 2026 AT 00:02Henri-Paul Soulodre
June 11, 2026 AT 20:53Mark Hogan
June 13, 2026 AT 17:01